Writing in Social Gerontology
How is Gerontology Positioned in Relation to Other Disciplines?
Figure 1: Social Gerontology and Fields with Which It Shares Connections.
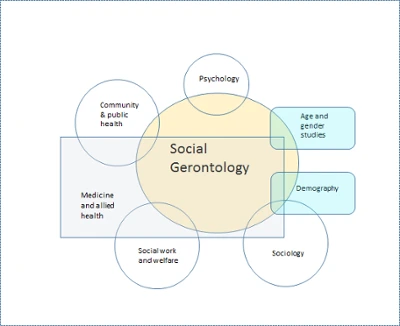
The image above "Social Gerontology" appears in a beige circle in the middle of the figure: the names of other fields appear in shapes that surround and overlap with Social Gerontology. Starting at the top and moving clockwise are the following fields: psychology, age and gender studies (also overlaps with medicine and allied health), demography (also overlaps with sociology and medicine and allied health), sociology (also overlaps with demography and medicine and allied health), social work and welfare (also overlaps with medicine and allied health), medicine and allied health (also overlaps with age and gender studies; demography; sociology; social work and welfare; and community and public health), and community and public health (also overlaps with medicine and allied health)
Figure 2: Visualization of Influential Theorists/Researchers in the Field of Social Gerontology.

The image above is of influential theorists/researchers stacked on top of each other. The names are in different colors over a black background. The names from top to bottom are as follows: Lawton, Kent, Bengston, Dannefer, Ferraro, Rubinstein, Cole, Hudson, Elder, Baltes, Achenbaum, Ray, Holstein, Binstock, Settersten, Gubrium, Birren, Schaie, Hendricks, Carstensen, Havinghurst, and Neugarten.
How Does all of this Manifest in Writing?
The article below shows examples of conventions of writing in Gerontology in context, specifically:
- what constitutes “respectful authority” in Gerontological writing
- how signposting manifests in Gerontology
- the significance of using descriptive headers
- how most Gerontological work draws on diverse sources from relevant disciplines
This guide was co-created by HCWE graduate assistant Angela Glotfelter and Gerontology faculty Dr. Suzanne Kunkel, Dr. Kate de Medeiros, and Dr. Jennifer Kinney.
Annotated Sample of Writing from Social Gerontology
The following are sections from an academic article from the field of Gerontology. Miami faculty from Gerontology have inserted comments to point out places that show disciplinary writing conventions in gerontology. These comments appear within the text of the article and are noted with bold text, brackets [], and the word "comment." Some sections of the original article have been removed for space, and this information is also noted with bold text and brackets.
The following is an academic article from the field of Gerontology. Miami faculty from Gerontology have inserted comments to indicate and explain disciplinary writing conventions in Gerontology.
This sample contains 13 comments. These comments appear within the text of the article and are noted with bold text, brackets [ ], and the word "comment." Some sections of the original article have been removed for space, and this information is also noted with bold text and brackets. You can also view these annotations or the original article in other formats linked below:
Linda Clare, Ph.D., Julia Rowlands, MSc, Errollyn Bruce, MA, Claire Surr, Ph.D., and Murna Downs, Ph.D. The Gerontologist, Volume 48, Issue 6, 1 December 2008, Pages 711–720
An accumulating body of evidence provides valuable insights into the subjective experience of living with early-stage dementia in community settings. We have known for some time that the subjective experience of people with moderate to severe dementia is less well delineated (Downs, 1997), although it is increasingly accepted that people in the middle to late stages of dementia retain the capacity for emotional expression (Magai, Cohen, Gomberg, Malatesta, & Culver, 1996) and many can reliably report aspects of their own experience, such as mood (Kolanowski, Litaker, & Catalano, 2002) or quality of life (Logsdon, Gibbons, McCurry, & Teri, 1999; Thorgrimsen et al., 2003).
Although the subjective meaning of aspects of living and dying in residential care has been explored in a number of studies (e.g., Gubrium, 1993; Kayser-Jones, 2002), these studies do not focus specifically on people with dementia. [Comment 1: This first sentence is an example of respectful authority. This comment acknowledges (positively) the past research but respectfully points to gaps in knowledge.] The experience of dementia has been widely explored in personal accounts and interview-based qualitative studies, but these have largely focused on people who have early-stage dementia and are living in the community. [Comment 2: The second half of the previous sentence is an example of signposting] A number of personal accounts vividly describe the impact of developing dementia (Lee, 2003; Snyder, 1999; Taylor, 2006). Qualitative researchers have attempted to capture the essential elements of this experience. Steeman, de Casterlé, Godderis, and Grypdonck (2006) identified 28 qualitative studies published between 1990 and 2004 that merited inclusion in their comprehensive review, mostly utilizing variants of grounded theory (e.g., Harris & Sterin, 1999; Keady & Nolan, 2003; Menne, Kinney, & Morhardt, 2002) or phenomenological methods (e.g., Clare, 2002, 2003; Phinney, 2002; Phinney & Chesla, 2003).
Studies using direct accounts and interviews as a means of understanding the subjective experience of living with moderate to severe dementia are rare. [Comment 3: Another example of respectful authority. The authors don't say that "no studies exist" or use language that is value laden.] To date, the understanding of the experience of people with moderate to severe dementia is largely derived from observational and questionnaire-based studies. A number of observational studies provide an insight into the experience of life for people with moderate to severe dementia in residential care homes or hospital units (Barnett, 2000; Perrin, 1997; see also Brooker, 2005). Perrin found minimal levels of well-being and a lack of meaningful occupation. Lack of meaningful occupation was also reported by Cohen-Mansfield, Marx, and Werner (1992). Ethnographic studies describe a complex framework of social interaction, both verbal and nonverbal, among care home residents (Hubbard, Cook, Tester, & Downs, 2002; Hubbard, Tester, & Downs, 2003; Kontos, 2004). The extent to which selfhood or identity is preserved has been an important focus in many of these observational studies, with results suggesting that although the self is affected by dementia, manifestations of selfhood do persist even in severe dementia (Small, Geldart, Gutman, & Scott, 1998; Tappen, Williams, Fishman & Touhy, 1998), along with the capacity to develop positive and therapeutic relationships (Williams & Tappen, 1999). Questionnaire-based studies have also begun to address this issue; for example, recent studies have elicited information from residents, staff, and family members about residents' occupational and family roles and preferred activities, concluding that aspects of identity were preserved even in severe dementia (Cohen-Mansfield, Golander, & Arnheim, 2000; Cohen-Mansfield, Parpura-Gill, & Golander, 2006a, 2006b).
A few studies have attempted to seek the perspectives of people with moderate to severe dementia on specific issues such as factors relating to quality of life and quality of care, or to use residents' own accounts to address specific aspects of experience such as preservation of selfhood or the meaning of disturbing behavior. The need to consider multiple perspectives, including those of the residents themselves, has been emphasized in relation to understanding quality of life by Sloane and colleagues (2005) and by Edelman, Fulton, Kuhn, and Chang (2005). It has been suggested that residents with severe dementia show some awareness of cognitive decline alongside indications of preserved selfhood (Mayhew, Acton, Yauk, & Hopkins, 2001). Recurrent issues of loss, communication difficulties, frustration, and sadness, along with various attempts to cope, have been highlighted in several studies (Aggarwal et al., 2003; Barnett, 2000). Relationships and desirable social roles, for example being part of a family, seem central to the preservation of self, although the ability to create narratives about one's life and past experiences is also important (Surr, 2006).
In their attempts to elicit the views of care home residents with dementia about the care they receive, researchers have identified dissatisfaction with lack of activities and social contact, and lack of choice and independence, as important (Aggarwal et al., 2003; Train, Nurock, Manela, Kitchen, & Livingston, 2005). Graneheim and Jansson (2006) described residents said to display disturbing behavior as feeling surrounded by disorder and trapped by restriction, leading to the conclusion that disturbing behavior could be seen as a way of communicating one's story and maintaining a self within the residential care context.
Although these studies have provided valuable information, research on the experience of living with dementia in long-term care that is based on direct accounts from the person with dementia remains rare. [Comment 4: This first sentence is another great example of sign posting. The authors reiterate that there has been great work but that studies on this particular topic are rare, which signals the introduction of their argument.] Focusing on predefined constructs such as experiences of care, preservation of selfhood, or the meaning of disturbing behavior, although relevant and useful, provides a specific, delineated perspective shaped by particular research questions. In the present study, we aimed to take a broader approach to understanding the experience of living with dementia in long-term care, focusing in particular on people with moderate to severe dementia, by examining accounts elicited directly from the residents themselves. We set out to explore the subjective experience of life with dementia in residential care in a large sample of residents, to understand the psychological impact of being in this situation, and to develop a thematic framework for making sense of this experience that could contribute to improving quality of life and quality of care.
[The middle sections of this article have been removed.]
[Comment 5: The sections in the original article contained subheadings to organize information, which is important in the field of gerontology]
[Comment 6: Diverse disciplines; mostly peer-reviewed journal articles (which hold the highest weight by far.) A good percentage come specifically from gerontology. Very few books (which are viewed as lest robust sources depending on the topic.)]
[Comment 7: A journal from nursing] Aggarwal, N., Vass, A., Minardi, H., Ward, R., Garfield, C., & Cybyk, B., (2003). People with dementia and their relatives: Personal experiences of Alzheimer's and of the provision of care. Journal of Psychiatric and Mental Health Nursing, 10, 187-197.
[Comment 8: A journal from medicine] Ballard, C., Fossey, J., Chithramohan, R., Howard, R., Burns, A., & Thompson, P., et al (2001). Quality of care in private sector and NHS facilities for people with dementia: Cross-sectional survey. British Medical Journal,323, 426-427.
Barnett, E. (2000). Including the person with dementia in designing and delivering care. London: Kingsley.
[Comment 9: A journal from gerontology] Brooker, D., (2005). Dementia care mapping: A review of the research literature. The Gerontologist, 45, (Special Issue 1), 11
-18.
Bruce, E., Surr, C., & Tibbs, M. A., (2002). A special kind of care: Improving well-being in people living with dementia. Derby: MHA Care Group.
[Comment 10: A journal from gerontology] Clare, L. (2002). We'll fight it as long as we can: Coping with the onset of Alzheimer's disease. Aging and Mental Health, 6, 139-148.
Clare, L. (2003). Managing threats to self: Awareness in early-stage Alzheimer's disease. Social Science and Medicine, 57, 1017-1029.
[Comment 11: A journal from social science] Cohen-Mansfield, J., Golander, H., & Arnheim, G., (2000). Self-identity in older persons suffering from dementia: Preliminary results. Social Science and Medicine, 51, 381-394.
Cohen-Mansfield, J., Marx, M. S., & Werner, P., (1992). Observational data on time use and behaviour problems in the nursing home. Journal of Applied Gerontology, 11, 111-121.
[Comment 12: A journal from gerontology] Cohen-Mansfield, J., Parpura-Gill, A., & Golander, H., (2006). Utilisation of self-identity roles for designing interventions for persons with dementia. Journal of Gerontology: Psychological Sciences,61B, P202-P212.
Cohen-Mansfield, J., Parpura-Gill., A., & Golander, H., (2006). Salience of self-identity roles in persons with dementia: Differences in perceptions among patients themselves, family members and caregivers. Social Science & Medicine,62, 745-757.
Downs, M., (1997). The emergence of the person in dementia research. Ageing and Society,17, 597-607.
Edelman, P., Fulton, B. R., Kuhn, D., & Chang, C-H., (2005). A comparison of three methods of measuring dementia-specific quality of life: Perspectives of residents, staff and observers. The Gerontologist,45, (Special Issue 1), 27-36.
[Comment 13: A journal from psychology] Elliott, R., Fischer, C. T., & Rennie, D. L. (1999). Evolving guidelines for publication of qualitative research studies in psychology and related fields. British Journal of Clinical Psychology,
38, 215-229.
[The rest of the References have been removed]
Howe Writing Center
